How to Choose the Right Preclinical Model for Kidney Disease Drug Development?
Selecting the right preclinical model is one of the most important decisions in a kidney drug development program.
A model determines which disease mechanisms can be reproduced, which efficacy endpoints can be measured and how confidently the results can support the next development decision. Even a technically successful study may provide limited value if the experimental model is not aligned with the candidate’s mechanism of action or the intended clinical indication.
There is no single model that reproduces every component of human kidney disease. The most appropriate strategy is therefore not to identify the “best” renal model in absolute terms, but to select the model or combination of models, that best answers a clearly defined development question.
Start with the biological question
Before choosing an experimental system, the project team should define what the study must demonstrate.
Typical objectives include:
- showing protection against acute tubular injury;
- limiting inflammation after an ischemic or toxic insult;
- preventing maladaptive repair and the transition from acute kidney injury to chronic kidney disease;
- reducing extracellular matrix accumulation and renal fibrosis;
- preserving glomerular or tubular function;
- identifying a potential nephrotoxicity signal;
These objectives are related, but they are not interchangeable. A model that provides a rapid and robust fibrotic response may not provide an informative measurement of renal function. Conversely, a model designed to generate a strong functional impairment may introduce mortality, variability or systemic effects that complicate the interpretation of tissue-specific activity.
The study question should therefore be translated into a predefined biological hypothesis. For example:
“Does the candidate reduce early tubular injury following ischemia?”
This question requires a different experimental design from:
“Does the candidate prevent the development of fibrosis after incomplete recovery from acute kidney injury?”
Match the model to the intended disease process
Ischemia-reperfusion injury models
Renal ischemia-reperfusion injury, or IRI, is commonly used to investigate acute tubular damage, inflammation, repair and progression towards chronic lesions.
The experimental outcome depends strongly on the design. Important variables include whether the injury is unilateral or bilateral, the duration of ischemia, the reperfusion period and whether the contralateral kidney remains functional.
A unilateral IRI model can be useful for studying local tissue injury, inflammation and fibrosis over time. The unaffected kidney supports survival and compensates for the injured kidney, but this compensation can make circulating functional biomarkers less sensitive.
Bilateral IRI affects the total renal functional reserve and may consequently produce clearer systemic changes. However, the model can also be associated with greater mortality, increased variability and a narrower window between insufficient and excessive injury.[1,2]
For studies focusing on the transition from acute injury to chronic kidney disease, unilateral IRI may be combined with contralateral nephrectomy. The timing of the nephrectomy can be adapted to create functional stress while allowing the initial injury and repair response to develop. This type of design can support the evaluation of fibrosis, inflammation and residual function, although the additional surgical procedure increases experimental complexity.[3]
UUO Model – Unilateral Ureteral obstruction model
Unilateral ureteral obstruction, or UUO, produces rapid tubular injury, inflammation, fibroblast activation and extracellular matrix accumulation. It is widely used to evaluate anti-fibrotic mechanisms and tissue markers such as collagen, fibronectin and α-smooth muscle actin.[4]
Its principal advantage is the rapid and reproducible development of tubulointerstitial fibrosis. However, the unobstructed kidney maintains overall renal function. Plasma creatinine and blood urea nitrogen may therefore provide limited information about the severity of injury in the obstructed kidney.
UUO is particularly relevant when the main objective is to investigate tissue remodeling or demonstrate activity against a defined pro-fibrotic pathway. It may be less appropriate when preservation of whole-organ function is the primary efficacy claim.
Diabetic kidney disease model
Models of diabetic kidney disease may be induced chemically, developed in genetically susceptible animals or combined with additional interventions that accelerate renal injury.
The STZ Model – Streptozotocin-induced diabetes – can reproduce sustained hyperglycemia and selected renal manifestations of diabetic disease. Genetically diabetic models provide a different metabolic and disease context. In some designs, uninephrectomy or dietary interventions are added to accelerate renal alterations.
These models may be appropriate for candidates targeting hyperglycemia-associated inflammation, oxidative stress, albuminuria, glomerular injury or progressive fibrosis. Their main limitations are generally their duration, the influence of metabolic variability and the need to distinguish direct renal effects from broader effects on glucose control or body weight.[5]
Nephrotoxicity models
Compounds such as cisplatin are frequently used to induce acute tubular injury and evaluate nephroprotective strategies.
These models can generate measurable changes in renal function, urinary injury biomarkers, histology and gene expression. However, dose, administration schedule, hydration, animal characteristics and study duration can strongly affect injury severity. Systemic toxicity must also be monitored, since severe general toxicity may complicate the interpretation of kidney-specific effects.
A nephrotoxicity model should therefore be selected and calibrated according to the intended use: mechanistic investigation, biomarker qualification, compound protection or safety assessment.
Define the required endpoints before finalizing the model
Model selection and endpoint selection should be performed together.
Functional endpoints
Common functional measurements include:
- plasma creatinine; blood urea nitrogen; glomerular filtration measurements; albuminuria or proteinuria;
Functional endpoints are especially valuable when the study is intended to demonstrate preservation of kidney performance. Their sensitivity nevertheless depends on the model. In unilateral injury models, compensation by the unaffected kidney can mask substantial tissue damage.
Injury and disease biomarkers
Urinary or plasma biomarkers can detect biological changes that are not fully captured by conventional renal function parameters. Depending on the model and injury compartment, relevant biomarkers may include KIM-1, NGAL, cystatin C, albumin and inflammatory mediators.
Biomarkers should be selected according to the expected location and timing of injury. A candidate targeting early tubular stress, for example, may require different sampling times from a candidate intended to prevent late fibrotic remodeling.
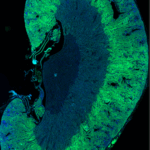
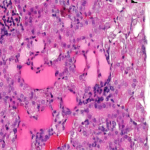
Histology and immunofluorescence
Histological analysis provides spatial information that cannot be obtained from plasma or urine alone.
Depending on the study objective, tissue analysis may include:
- tubular injury scoring;
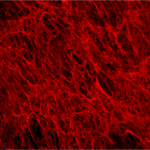
- extracellular matrix staining or collagen quantification;
- inflammatory-cell infiltration;
- myofibroblast activation;
- glomerular or tubular structural alterations.
Digital image analysis can strengthen objectivity and improve the reproducibility of tissue quantification, provided that sampling, staining, image acquisition and analysis criteria are standardized before the study begins.
Gene and protein expression
Gene-expression and protein analyses can confirm target engagement and characterize the effect of treatment on injury, inflammation, fibrosis or repair pathways.
These endpoints are particularly useful when integrated with functional and histological findings. A change in a single molecular marker may support a mechanistic hypothesis, but it is usually insufficient on its own to demonstrate a meaningful renal benefit.
Account for timing and treatment strategy
Kidney injury evolves over time. Early phases may be dominated by cell stress, necrosis and innate immune activation, whereas later phases may involve repair, persistent inflammation, fibroblast activation and matrix deposition.
The appropriate study duration therefore depends on the candidate’s intended effect.
A preventive treatment may begin before or immediately after injury. A therapeutic design should generally begin after the pathological process has been initiated. This distinction is essential: a compound that prevents the initial insult may not necessarily reverse an established disease process.
Sampling time points should also reflect the expected pharmacology. Early samples may be needed to confirm target engagement, while later samples may be required to demonstrate structural or functional benefit.
Consider the source of experimental variability
Several variables can materially influence renal model outcomes:
- species, strain, sex and age;
- baseline randomization and metabolic status;
- housing and acclimation;
- surgical technique and operator experience;
- procedure duration;
- anesthesia, analgesia and temperature control;
- formulation and route of administration;
- sample collection procedures and analytical methods.
These variables should not be treated as minor operational details. They are part of the biological model and should be controlled through standardized procedures, appropriate randomization, predefined exclusion criteria and blinded analyses whenever feasible.
Use a staged model strategy
For many programs, the strongest approach is not a single large efficacy study but a sequence of complementary experiments.
Stage 1: Human-relevant in vitro screening
Human renal cells or co-culture systems can be used to:
- compare compounds and concentrations;
- assess cytotoxicity;
- investigate mechanism of action;
- identify pharmacodynamic biomarkers;
- select candidates for in vivo studies.
In vitro systems allow efficient experimental control and can reduce the number of compounds entering animal studies. However, they do not reproduce whole-organ physiology, systemic exposure or interactions between the kidney and other organs.
Stage 2: Focused in vivo proof of concept
The in vivo model should test the most important remaining development question. Treatment groups, doses, sampling times and endpoints should be selected based on the in vitro results, pharmacokinetic information and expected mechanism of action.
Stage 3: Translational confirmation
A subsequent study may use a second model, a therapeutic treatment design, an additional species or a broader biomarker panel. This can determine whether the observed effect is robust across different pathological contexts rather than being specific to a single experimental condition.
Conclusion
The value of a preclinical kidney study depends on the alignment between the therapeutic hypothesis, experimental model, treatment schedule and endpoint strategy.
A robust model is not simply one that generates severe kidney injury. It is one that produces interpretable biological changes at the appropriate time, with acceptable variability and a clear relationship to the candidate’s intended mechanism and clinical application.
NEPHRIX Biosolutions supports pharmaceutical and biotechnology companies in the design and execution of customized renal studies using complementary in vitro, in vivo, biomarker and histology approaches.
Planning a preclinical kidney efficacy study? Contact our scientific team to discuss the most appropriate model and endpoint strategy for your candidate.
Selected references
- Godoy JA, Watson G, Raspante C, Illanes O. An Effective Mouse Model of Unilateral Renal Ischemia-Reperfusion Injury. Journal of Visualized Experiments. 2021;(173):e62749. doi: 10.3791/62749.
- Arvaniti E, Moulos P, Vakrakou A, Chatziantoniou C, Chadjichristos C, Kavvadas P, Charonis A, Politis PK. Whole-transcriptome analysis of UUO mouse model of renal fibrosis reveals new molecular players in kidney diseases. Scientific Reports. 2016;6:26235. doi: 10.1038/srep26235..
- Hudkins KL, Pichaiwong W, Wietecha T, et al. BTBR Ob/Ob mutant mice model progressive diabetic nephropathy. Journal of the American Society of Nephrology. 2010;21(9):1533–1542. doi: 10.1681/ASN.2009121290.
- Ma Z, Hu X, Ding HF, Zhang M, Huo Y, Dong Z. Single-Nucleus Transcriptional Profiling of Chronic Kidney Disease after Cisplatin Nephrotoxicity. American Journal of Pathology. 2022;192(4):613–628. doi: 10.1016/j.ajpath.2021.12.012.
- Lu W, Phillips CL, Killen PD, Hlaing T, Harrison WR, Elder FFB, Miner JH, Overbeek PA, Meisler MH. Insertional mutation of the collagen genes Col4a3 and Col4a4 in a mouse model of Alport syndrome. Genomics. 1999;61(2):113–124. doi: 10.1006/geno.1999.5943.
Recent Posts