Kidney Disease biomarkers beyond Creatinine
GFR and serum creatinine detect kidney damage only after nearly 50% of function is lost.
At NEPHRIX Biosolutions, we routinely measure next-generation biomarkers, KIM-1, NGAL, BUN and more, across all nephron segments to give your program the sensitivity it needs.
Assessment of kidney function and disease progression have mainly focused on the evaluation of 2 biological standards: the glomerular filtration rate (GFR) and serum creatinine levels.
As kidney diseases are complex and heterogeneous, these parameters omit to evaluate the kidney tubular health and allow a late detection of disease progression only. Therefore, restraining the investigation of kidney disease on these 2 parameters limit the development and evaluation of therapeutic strategies to minimize kidney injury at the early stages of the disease course.
These last years, several new biomarkers have been described with a potential to better determine the clinical health of the different nephron segments and applied from acute to chronic kidney diseases. On the scheme below, we listed some renal specific parameters that we assess in routine in our different experimental systems.
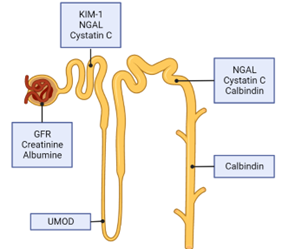
Renal Biomarkers at a Glance
All biomarkers below are assessed in routine in our experimental systems, across both in vitro and in vivo models.
| Biomarker | Compartment | Disease phase | Human normal | Detection speed |
|---|---|---|---|---|
| GFR (sinistrin) | Glomerular | AKI + CKD | 0.15–2 mL/min/100g BW | Moderate |
| Creatinine | Glomerular / systemic | CKD | 0.6–1.3 mg/dL | Late (>50% loss) |
| KIM-1 | Proximal tubule | AKI CKD | <1 ng/mL | Early |
| BUN | Systemic (protein metabolism) | AKI + CKD | 6–24 mg/dL | Moderate |
| NGAL | Proximal & distal tubule | AKI | ≤50 ng/mL (urine) | Very early (<2h) |
Glomerular Filtration Rate (GFR)
It is calculated by measuring any chemical that has a stable level in the blood and is freely filtered but neither reabsorbed nor secreted by the kidneys. Clinically, blood levels measurement of inulin after injection is still considered as the gold standard for the estimation of GFR. In case of chronic kidney disease or reduction of renal mass, the GFR is reduced that is paralleled with the organ loss of function.
The evaluation of GFR in preclinical experimental models can be performed via the MediBeacon® Patches Technology. This procedure is based on intravenous injection of a fluorescent tracer allowing the evaluation of its blood levels across the animal skin. This strategy avoids the repetitive blood sampling and animal restraining during the monitoring.
Creatinine
Creatinine is a waste product left over from energy-producing processes in muscles. Kidneys filter creatinine from the blood to the urine. In case of kidneys damage, creatinine accumulates in the blood and less is released in urine. The ratio between blood and urine creatinine levels is an effective parameter to detect signs of kidney disease.
However, the evaluation of kidney function via creatinine levels only shows several limitations as this biomarker is influenced by multiple factors extrinsic to the kidney (ie, age, sex, muscle mass, metabolism, diet, medications, hydration status…). Furthermore, levels of creatinine do not rise until nearly 50% of kidney function is damaged, leading to inaccurate chronic kidney disease staging and false negatives.
Blood Urea Nitrogen (BUN)
Blood Urea Nitrogen (BUN) is a serum waste product of protein metabolism. This product is filtered by the kidneys and removed from the body in urine. Elevations in BUN levels in the blood are often, but not always, a result of a decrease in GFR. Some factors enhance urea production, such as gastrointestinal bleeding, corticosteroid therapy, or high-protein diet, and limit the utility of BUN in assessing kidney function in these specific conditions.
Neutrophil Gelatinase-Associated Lipocalin (NGAL)
NGAL is a 25 kDa glycoprotein expressed and secreted by proximal and distal renal tubular cells. The NGAL biomarker has been considered as the most promising biomarker of acute kidney injury (AKI) as it rises rapidly (within 2 hours) in response to kidney injury.
This protein plays important roles in nephron recovery during infection, inflammation, due to nephrotoxic drugs. Serum and urinary NGAL have similar sensitivity for assessing renal damage. However, the overall pathologic conditions, like inflammation, sepsis or cancer also upregulate NGAL levels, which may blur the accuracy of NGAL as renal damage indicator.
Normal urinary range:
About us – NEPHRIX Biosolutions, the leading kidney disease CRO
NEPHRIX Biosolutions is a specialist preclinical contract research organisation (CRO), dedicated exclusively to kidney disease research. Unlike generalist CROs that adapt standard models to renal endpoints, every platform, assay, and protocol at NEPHRIX has been designed from the ground up around nephrology.
Our team brings together expert renal biologists, histopathologists, and translational scientists with a shared focus on accelerating the development of new therapies for acute kidney injury (AKI), chronic kidney disease (CKD), diabetic nephropathy, and renal fibrosis.
From first-in-class compound screening to IND-enabling studies, we partner with biotech and pharma teams at every stage, providing reproducible, publication-quality data with fast turnaround and direct access to our scientific team.